Purpose:
To guide therapists on what to document in the Interventions/Goals section for a routine visit.
Question Intent:
Per Medicare Benefit Policy Manual Chapter 7 - Home Health Services, the Interventions/Goals section highlights the importance “that the home health records for every visit will reflect the need for skilled medical care provided.”
It is a requirement that documentation of patient care is skilled in nature to justify professional therapy services. The core of skilled documentation must answer the following on each note:
- What did the therapist teach, train and/or instruct on?
- What was the patient’s reaction/response to care as noted by demonstrating learning of the training? (Teach Back)
- What is the status of the care related to patients progress towards goals?
The Show Details content for each Intervention/Goal is now organized so that as the clinician scrolls down the content comes in order of selection to make it easy to find and organize. In general, the information will be in the order of an (1) Introduction Visit Statement followed by (2) Content, and finally the (3) Concluding Statement. Below you will find step by step instructions and an example of this format with each section of information identified:
NOTE - see the Maintenance Therapy article to see how Interventions/Goals should be utilized for Maintenance Therapy patients.
Response-Specific Instructions:
- Click on Interventions/Goals in your visit note:
- Within Interventions/Goals are Categories. You will select each category to see specific Interventions to document to:
- Categories:
- Categories:
- Within the Category, specific Interventions that have been added by the Evaluating Therapist through 01 Pathways & New Order will appear. Below are some ADL examples:
- Whenever an Intervention is marked as Provided, the Show Details feature will be used:
- The Show Details options are organized so that as the clinician scrolls down, the content comes in order of selection to make it easy to find and organize. In general, the information will be in the order of an (1) Introduction Visit Statement followed by (2) Content, and finally (3) Concluding Statement. Below provides an example of this format with each section of information identified:
- It is required that three items from the Show Details are selected for every note. It is also required the therapist either 'free text' their skilled documentation, or use the pre-defined statements and customize accordingly. In summary, the Intervention Details should look like:
- Required - the (1) Introduction Visit Statement - Statement that begins the documentation and is found at the top of the Show Details list. There is generally one statement and focuses on what the therapist is teaching on.
- 2 options: (Required to do 1 or both)
- Option 1 - Free text skilled documentation. An example for grooming above may read:
- "in using 4ww with brakes locked to sit in front of bathroom mirror. Place hair brush within reach and brush with firm, short strokes to minimize tangles caught in brush."
- Option 2 - Pre-defined statements that are built in the (2) Content:
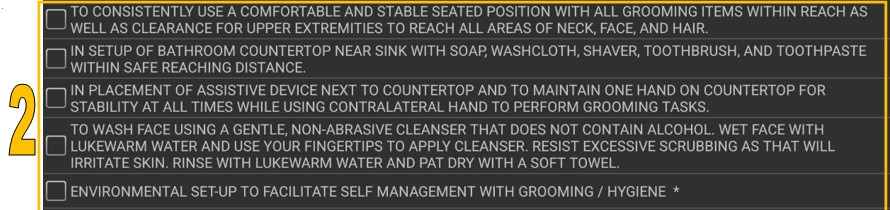
- The pre-defined statements are written as complete instructions and is intended to supplement a therapist’s unique patient note, but content should be changed to ensure the instructions are accurate by either adding or deleting sections that are not appropriate. It is not intended to be used in the fashion of cloning subsequent notes where there is identical verbatim language on every note. It is the responsibility of the clinician to make each note unique and defensible. Where appropriate, there are * to indicate where specific information needs to be added. If the content is left unaltered, the record defines the training provided was as exactly as written, so a therapist needs to be aware they will be held accountable to what is documented, if audited.
- Option 1 - Free text skilled documentation. An example for grooming above may read:
- Required - Teach Back statement from (2) Content:
- Required - (3) Concluding Statement - The final step is the conclusion of the intervention. The therapist will decide if they will continue (top 3 in screenshot) or discharge (bottom 3 in screenshot) based on patient progress. Discharge options should be reserved for when the Intervention Goal is marked as 'Met' or 'Not Met' at either the '33', '18', or '19'visits.
- Required - the (1) Introduction Visit Statement - Statement that begins the documentation and is found at the top of the Show Details list. There is generally one statement and focuses on what the therapist is teaching on.
- Here is an example of an OT selecting all required sections and using the pre-defined content for education/instructions:
- Once the asterisks are completed, this note would read as follows:











